Abstract
Kim Ann Ung, Richard Tsang, Melania Pintilie, David Hodgson, Alexander Sun, Vishal Kukreti, John Kuruvilla, Michael Crump, Mary Gospodarowicz
Princess Margaret Cancer Centre, Toronto, ON
Background: Prior to the widespread use of rituximab and CNS prophylaxis, testicular diffuse large B-cell lymphoma (DLBCL) was associated with poor prognosis. We examined the outcomes of patients treated between 1995 and 2010 to see if modern treatment improved the outcomes and specifically addressed the issue of CNS relapse.
Materials and Methods: A retrospective analysis of Stage I-II testicular DLBCL treated at our centre with combined modality therapy was performed. Survival and pattern of relapse were examined in detail.
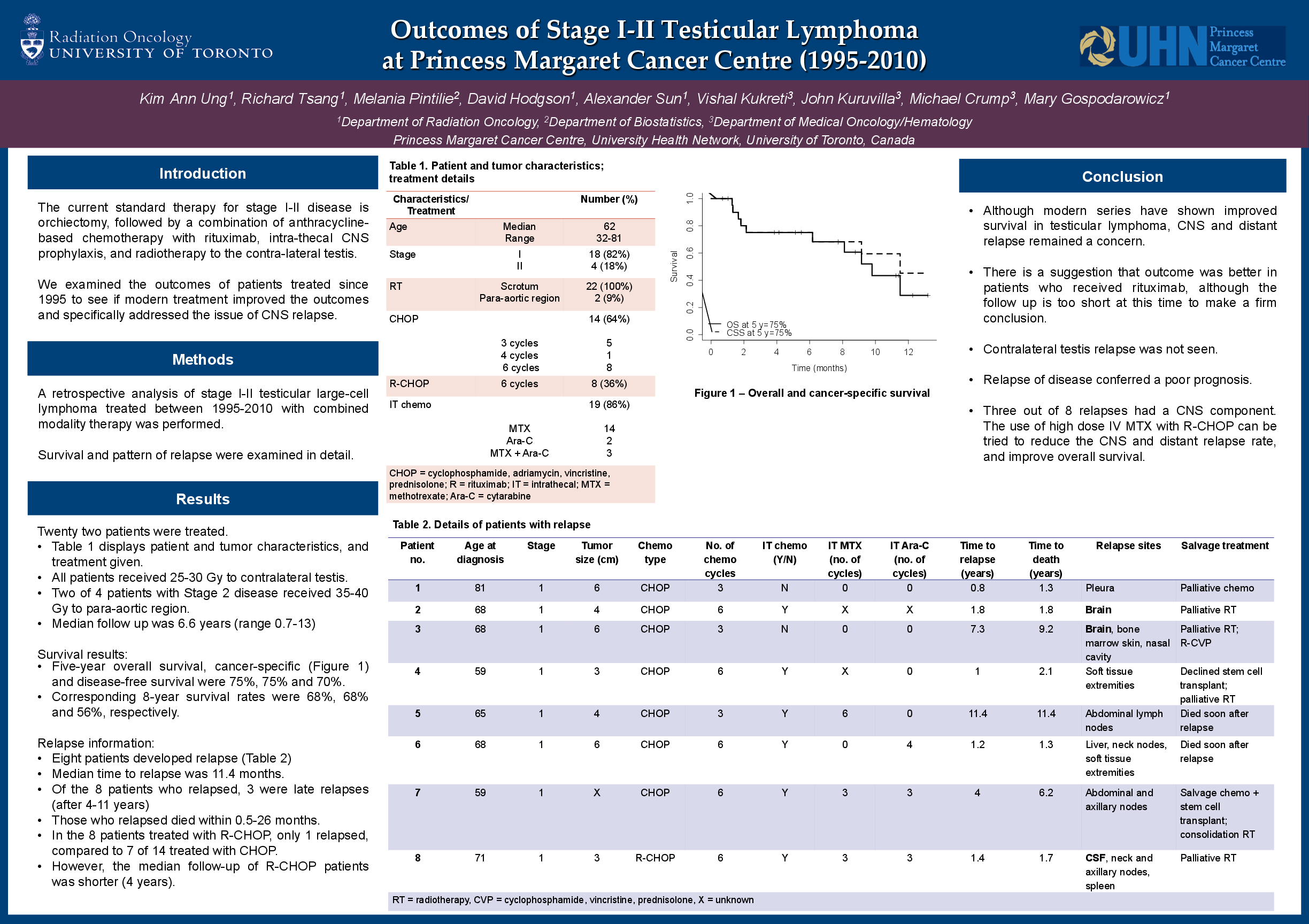
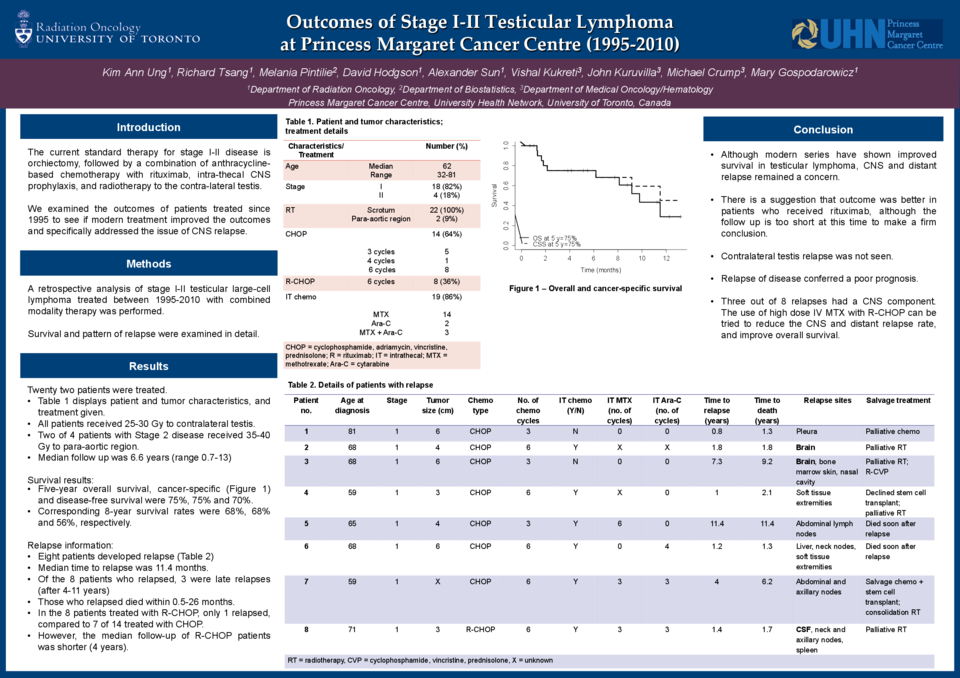
Results: Twenty-two patients were evaluated. Eighteen patients presented with Stage 1, and 4 with Stage 2 disease. Median age was 62 years (range 32-81). Fourteen patients received CHOP chemotherapy (3 cycles: five; 4 cycles: one; 6 cycles: eight) and eight patients received 6 cycles of rituximab (R) and CHOP. All patients received 25-35 Gy to contralateral testis. Nineteen patients received intrathecal chemotherapy (MTX +/- AraC, or AraC alone). Median follow up was 6.6 years (range 0.7-13). Five-year overall survival, cancer-specific and disease-free survival were 75%, 75% and 70%; and the corresponding eight-year survival rates were 68%, 68% and 56%, respectively. Median time to relapse was 11.4 months. Eight patients developed relapse, five in distant sites (eg. skin, spleen, liver), and three within CNS (one patient did not receive CNS prophylaxis). CNS relapse was observed as parenchymal disease in two patients, and meningeal involvement in one patient. Those who relapsed died within 0.5-26 months. In the eight patients treated with RCHOP, only one relapse was observed, compared to seven of 14 treated with CHOP. However, the median follow-up of these patients was shorter (four years).
Conclusions: Although modern series have shown improved survival in testicular lymphoma, CNS relapse remained a concern. We hope that the use of high dose IV MTX with RCHOP as per our current practice will reduce the CNS relapse rate. Contralateral testis relapse was not seen. Within this cohort, there is a suggestion that outcome was better in patients who received rituximab, although the follow up is too short at this time to make a firm conclusion. Relapse of disease conferred a poor prognosis