Abstract
DIFFUSE PARENCHYMAL LUNG DISEASE AS AN UNUSUAL MANIFESTATION OF IMMUNOGLOBULIN LIGHT CHAIN (AL) AMYLOIDOSIS
Akintunde Akinleye MBChB, MSc; Muhammad Furqan MD; Pavan Mahendra Ravella, MD
Division of Oncology/Hematology, Westchester Medical Center, Valhalla, New York.
P: 347 285 3535, email:
[email protected]
Case Presentation
A 78 year old Caucasian male presented with three months history of persistent, intermittent streaky hemoptysis. He denied any fevers, night sweats, chest discomfort, fatigue, bone pains or weight loss.
His examination revealed macroglossia, submandibular adenopathy and inspiratory crackles on lung auscultation. His laboratory tests showed hemoglobin 10g/dl, WBC 5.5/nl, platelet 273/nl, total protein 6.8g/dl, albumin 3.1g/dl, globulin 3.7g/dl and creatinine 0.7mg/dl. A chest radiograph showed bilateral interstitial markings and a normal-sized heart. His chest CT scan demonstrated bilateral diffuse interstitial infiltration with bibasilar opacities.
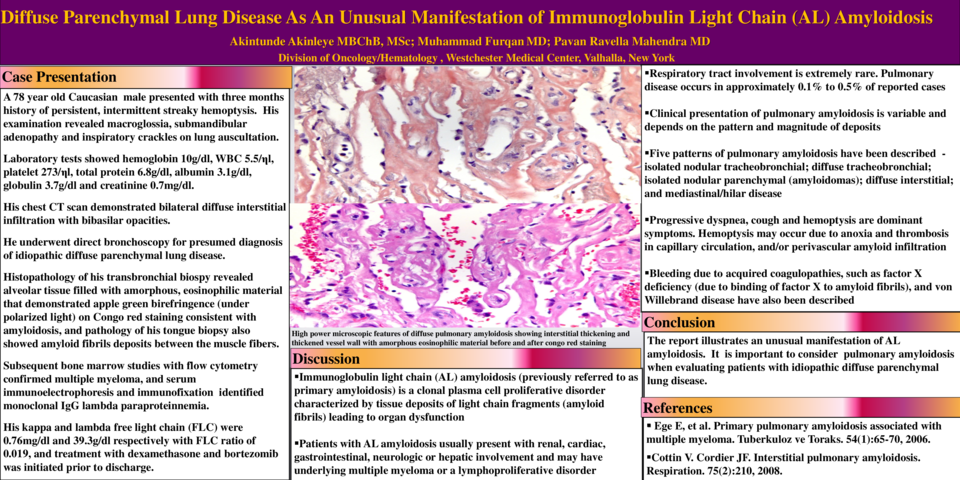
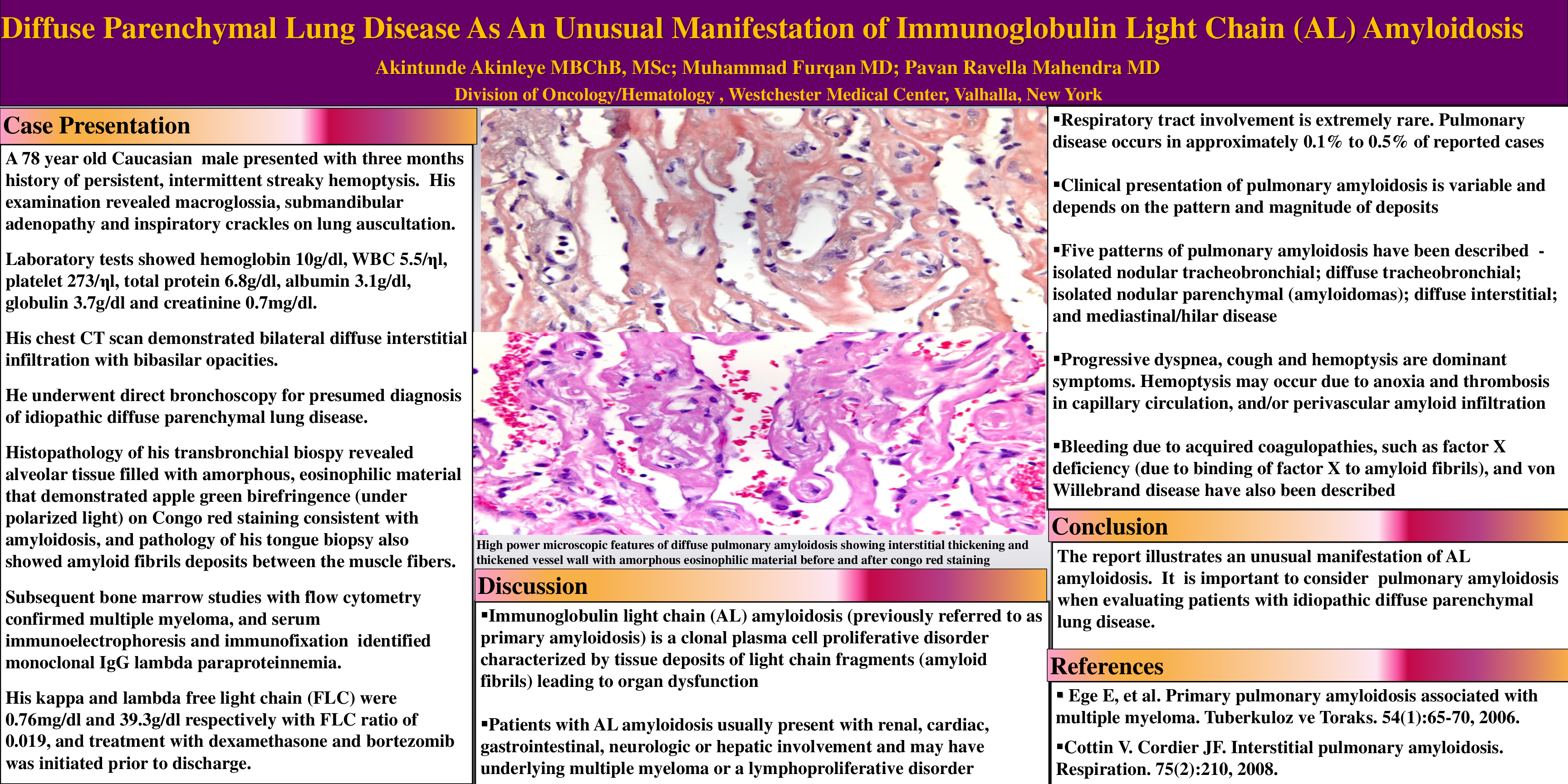
He underwent direct bronchoscopy for presumed diagnosis of idiopathic diffuse parenchymal lung disease. Histopathology of his transbronchial biospy revealed alveolar tissue filled with amorphous, eosinophilic material that demonstrated apple green birefringence (under polarized light) on Congo red staining consistent with amyloidosis, and pathology of his tongue biopsy also showed amyloid fibrils deposits between the muscle fibers. A subsequent bone marrow studies with flow cytometry confirmed multiple myeloma, and serum immunoelectrophoresis and immunofixation identified monoclonal IgG lambda paraproteinnemia. His kappa and lambda free light chain (FLC) were 0.76mg/dl and 39.3g/dl respectively with FLC ratio of 0.019, and treatment with dexamethasone and bortezomib was initiated prior to discharge.
Discussion and literature review
Immunoglobulin light chain (AL) amyloidosis (previously referred to as primary amyloidosis) is a clonal plasma cell proliferative disorder characterized by tissue deposits of light chain fragments (amyloid fibrils) leading to organ dysfunction. The fibrils are derived from the variable region of lambda light chains in approximately 75 percent of cases, and kappa in the remainder. Patients with AL amyloidosis usually present with renal, cardiac, gastrointestinal, neurologic or hepatic involvement and may have underlying multiple myeloma or a lymphoproliferative disorder. Respiratory tract involvement is extremely rare. Pulmonary disease occurs in approximately 0.1% to 0.5% of the reported cases of AL amyloidosis, and 5 patterns of manifestations (isolated tracheobronchial nodular deposits, diffuse tracheobronchial infiltration, isolated nodular parenchymal amyloidosis (amyloidomas), diffuse interstitial amyloidosis and mediastinal/hilar forms) have been described. The clinical presentation of pulmonary amyloidosis is variable and depends on the pattern and magnitude of deposits. However, progressive dyspnea, cough and hemoptysis are dominant symptoms. Hemoptysis may occur due to anoxia and thrombosis in capillary circulation, and/or perivascular amyloid infiltration of blood vessel which may lead to disruption of vessel wall and hemorrhage into the pulmonary interstitium. Bleeding due to acquired coagulopathies, such as factor X deficiency (due to binding of factor X to amyloid fibrils), and von Willebrand disease have been described in AL amyloidosis.
Conclusion
This report illustrates an unusual manifestation of AL amyloidosis in association with multiple myeloma presenting with persistent hemoptysis as a result of diffuse parenchymal deposition of amyloid fibrils. We suggest that AL amyloidosis should be considered when evaluating patients with idiopathic diffuse parenchymal lung disease.