White Matter Lesions in Term Infants with Neonatal Encephalopathy:Correlation with Later Scans and Neurodevelopmental Outcome
Abstract
Background:
The commonest brain abnormality following perinatal hypoxic-ischaemia (PHI) and neonatal encephalopathy (NE) is damage to the basal ganglia and thalami (BGT), which is associated with the development of cerebral palsy. A minority of infants presenting with NE have abnormality primarily in the white matter (WM). The long term MR brain scan findings and outcome of these children has not been well defined.
Aims:
To assess, in term infants with evidence of PHI and NE but without damage to the BGT
the evolution of MRI brain scans in the first 2 years
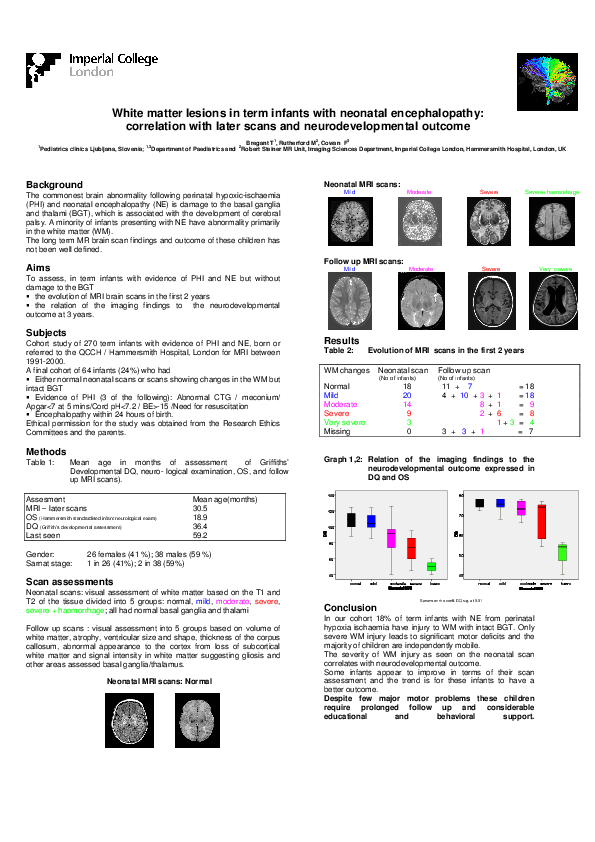
the relation of the imaging findings to the neurodevelopmental outcome at 3 years.
Subjects:
Cohort study of 270 term infants with evidence of PHI and NE, born or referred to the QCCH / Hammersmith Hospital, London for MRI between 1991-2000.
A final cohort of 64 infants (24%) who had
Either normal neonatal scans or scans showing changes in the WM but intact BGT
Evidence of PHI (3 of the following): Abnormal CTG / meconium/ Apgar<7 at 5 mins/Cord pH<7.2 / BE>-15 /Need for resuscitation
Encephalopathy within 24 hours of birth.
Ethical permission for the study was obtained from the Research Ethics Committees and the parents.
Methods:
Children were assessed at mean age MRI – later scans 30.5 months, optimality score was (Hammersmith standardised infant neurological exam) 18.9, DQ (Griffith’s developmental assessment) was 36.4. They were 26 females (41 %); 38 males (59 %); Sarnat stage: 1 in 26 (41%); 2 in 38 (59%)
Scan assessments:
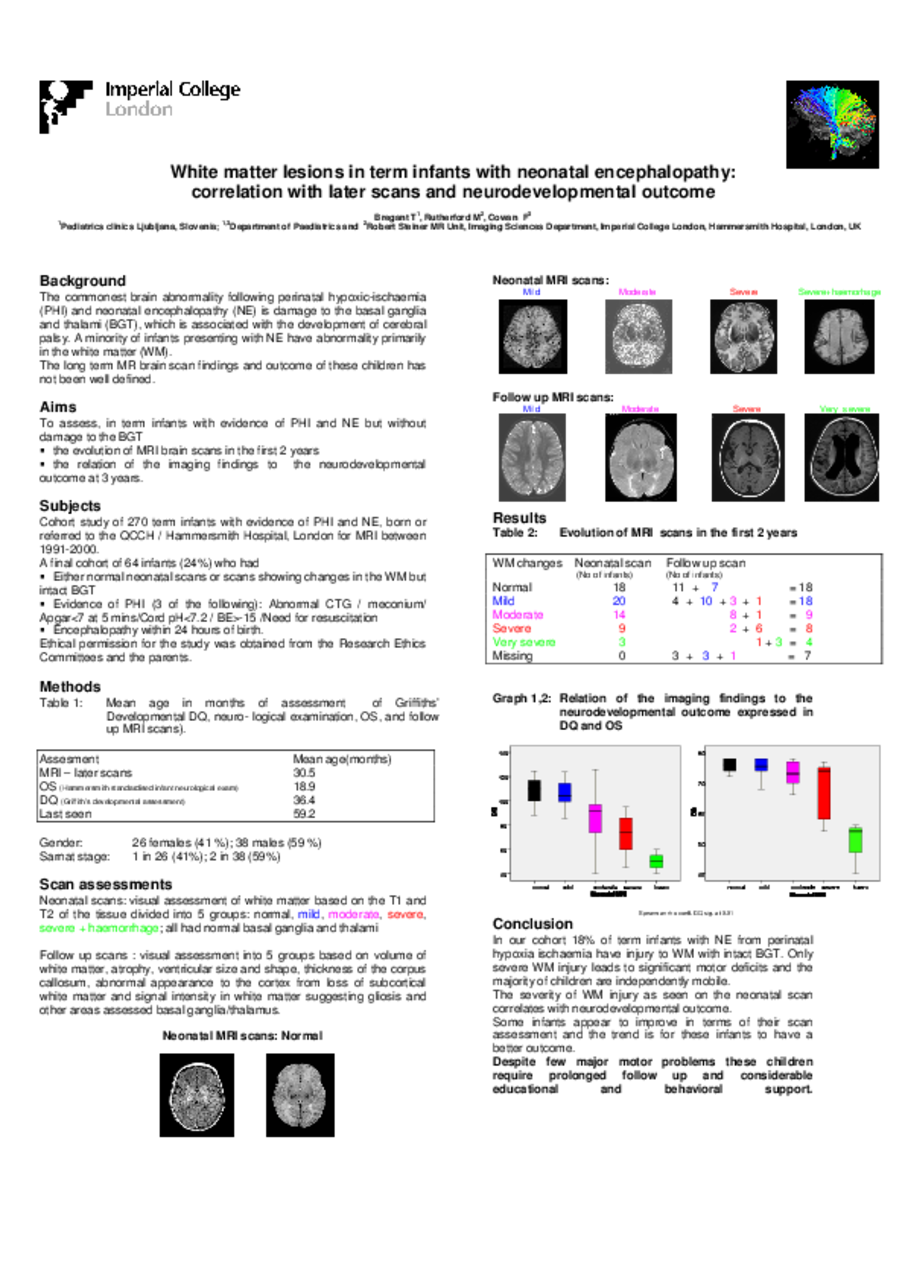
Neonatal scans: visual assessment of white matter based on the T1 and T2 of the tissue divided into 5 groups: normal, mild, moderate, severe, severe + haemorrhage; all had normal basal ganglia and thalami
Follow up scans: Visual assessment into 5 groups based on volume of white matter, atrophy, ventricular size and shape, thickness of the corpus callosum, abnormal appearance to the cortex from loss of subcortical white matter and signal intensity in white matter suggesting gliosis and other areas assessed basal ganglia/thalamus.
Results In 18 infants WM changes on neonatal scan were normal, from them on follow-up scan 7 were normal, 11 mild; 20 infants had on neonatal scans mild changes, while on their follow-up these changes were in 4 normal, 10 mild, 3 moderate and 1 severe; 14 infants had on neonatal scan moderate WM changes, while on follow-up 8 were moderate and 1severe; severe changes were seen perinatally in 9 infants, with their follow-up scans in 2 moderate and 6 severe; very severe changes were seen perinatally in 3 infants, with their follow-up scans rated as very severe in 3 and in 1 severe WM changes. 7 children were lost upon follow-up.
Conclusion:
In our cohort 18% of term infants with NE from perinatal hypoxia ischaemia have injury to WM with intact BGT. Only severe WM injury leads to significant motor deficits and the majority of children are independently mobile. The severity of WM injury as seen on the neonatal scan correlates with neurodevelopmental outcome.Some infants appear to improve in terms of their scan assessment and the trend is for these infants to have a better outcome.
Related articles