Non-Trauma Community Hospital Management of Head and Neck Wound from Alligator Bite
Abstract
Alligator attacks are uncommon and attacks that result traumatic neck injuries are even rarer. Traumatic penetrating neck wounds have a subjective treatment strategy based on the clinical picture of the patient and comfort level of the physician, but there is no specific algorithm. Traumatic injuries are typically treated by hospitals with a trauma center; however, in the following case, a penetrating neck injury caused by an alligator was treated at a local community hospital without a trauma center.
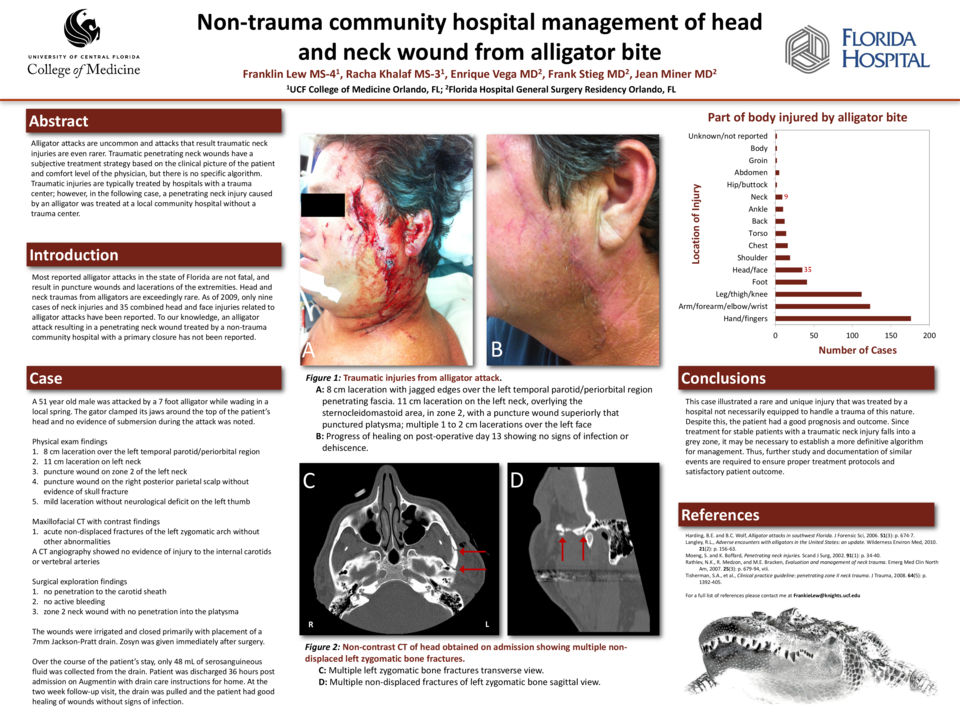
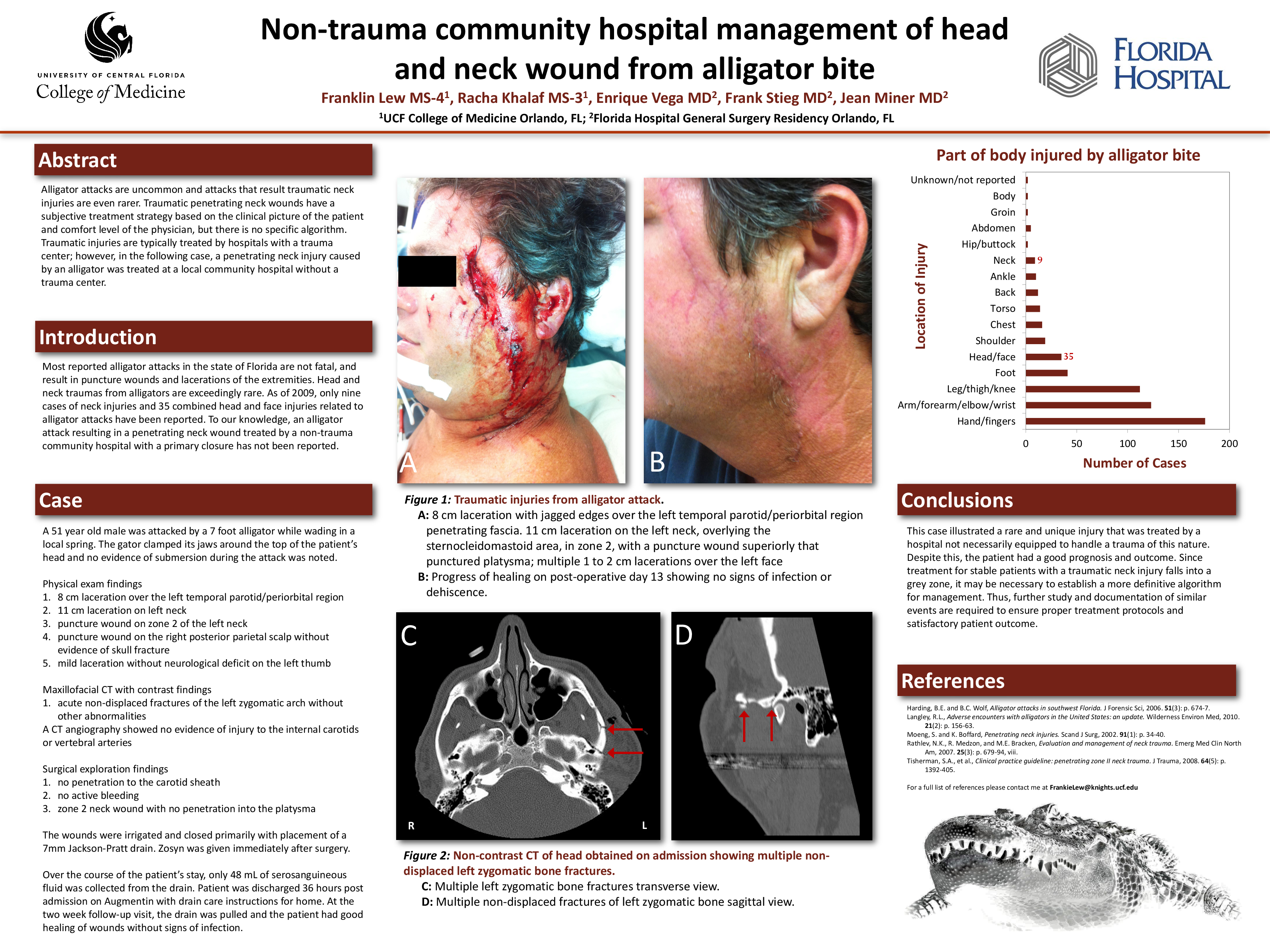
A 51 year old male was brought to our emergency department after being attacked by a 7 foot alligator while wading in a local spring. The gator clamped its jaws around the top of the patient’s head. No evidence of submersion during the attack was noted and the patient was able to escape and swim to safety. On physical exam a large 8 cm laceration over the left parotid area, puncture wound on zone 2 of the left neck, puncture on the right posterior parietal scalp without evidence of skull fracture, and a mild laceration without neurological deficit on his left thumb was observed. No other abnormalities noted. Labs only showed mild leukocytosis. A maxillofacial CT with contrast showed acute nondisplaced fractures of the left zygomatic arch without other abnormalities. A CT angiography was performed and showed no evidence of injury to the internal carotids or vertebral arteries. Surgical exploration was deemed necessary due to swelling of neck. The wounds of the left neck and face were explored in the trajectory of the puncture. The facial laceration was extended to the angle of the mandible and further explored. There was no penetration to the carotid sheath. No active bleeding was noted. The zone 2 neck wound was explored and noted to be relatively superficial with no penetration into the platysma. The wounds were irrigated and closed primarily with placement of a 7mm Jackson-Pratt drain. Zosyn was given immediately after surgery. Over the course of the patient’s stay, only 48 mL of serosanguineous fluid was noted from the drain. Patient was discharged 36 hours post admission on Augmentin with drain care instructions for home. On 2 week follow-up the drain was pulled and the patient had good healing of wounds without signs of infection.
This case illustrated a rare and unique injury that was treated by a hospital not necessarily equipped to handle this type of trauma that resulted in a good patient outcome. Since stable patients with a traumatic neck injury falls into a grey zone for treatment, it may be necessary to establish a more definitive algorithm for treatment. Thus further study and documentation of similar events is required to ensure proper treatment protocols and satisfactory patient outcome.
Related articles