Abstract
Introduction: Beaver tail liver is a rare hepatic anatomical variant in which the left hepatic lobe extends into the left upper quadrant and surrounds the spleen. The extension consists of normal hepatic parenchyma and involves no functional impairment. It is usually encountered in females and as an incidental finding on abdominal imaging. In cases of abdominal trauma to the upper left quadrant, the extended left hepatic lobe is more susceptible to injury and often confused for a splenic injury due to similar densities and echogenicities on ultrasound and CT.
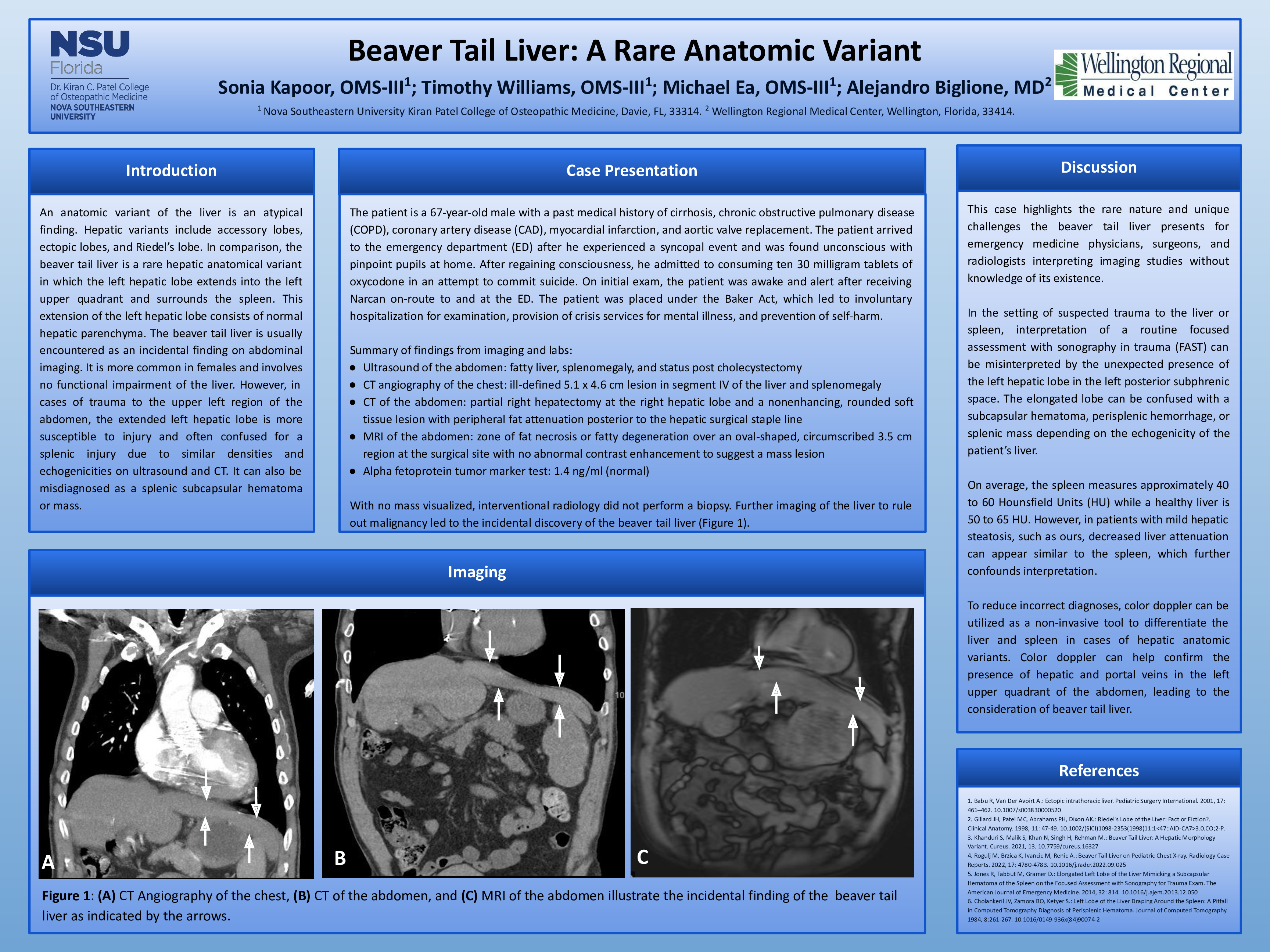
Case: The patient is a 67-year-old male with a past medical history of cirrhosis, chronic obstructive pulmonary disease, coronary artery disease, myocardial infarction, and aortic valve replacement. He arrived at the emergency room (ER) after he experienced a syncopal event and was found unconscious with pinpoint pupils at home. After regaining consciousness, he admitted he consumed ten 30 milligram tablets of oxycodone due to depression and an attempt to commit suicide. On initial exam, he was awake and alert after receiving Narcan onroute to and at the ER. Vitals on admission included a heart rate of 107 beats per minute, blood pressure of 156/69 mmHg, and 23 respirations per minute. The patient was placed under the Baker Act, resulting in involuntary hospitalization for examination and provision of crisis services for mental illness. Initially, abdominal ultrasound demonstrated a fatty liver, splenomegaly, and status post cholecystectomy. CTA of the chest revealed an ill-defined 5.1 x 4.6 cm lesion in segment IV of the liver. Alpha-fetoprotein tumor marker test was a normal level of 1.4 ng/ml. Abdominal CT showed partial right hepatectomy at the right hepatic lobe and a non-enhancing, rounded soft tissue lesion with peripheral fat attenuation posterior to the hepatic surgical staple line. Abdominal MRI confirmed a zone of fat necrosis or fatty degeneration over an oval-shaped, circumscribed 3.5 cm region at the surgical site with no abnormal contrast enhancement to suggest a mass lesion. Further imaging of the liver led to incidental discovery of the beaver tail liver. Upon completion of medical management, the patient was advised to follow up outpatient with gastroenterology and discharged to an inpatient psychiatric facility.
Discussion: Hepatic anatomic variants, such as accessory and ectopic lobes and Riedel’s lobe, are atypical findings. Beaver tail liver is uncommon and available literature is limited to many case reports describing it as an incidental finding. This case highlights the unique nature and challenges the beaver tail liver presents for emergency medicine physicians, surgeons, and radiologists interpreting imaging studies without knowledge of its existence. In cases of suspected hepatic or splenic trauma, a routine FAST exam can be misinterpreted due to an unexpected left hepatic lobe in the left posterior subphrenic space. It is also confused for a subcapsular hematoma, perisplenic hemorrhage, or splenic mass based on the echogenicity of the patient’s liver. On average, a spleen and healthy liver measure 40 to 60 HU and 50 to 65 HU, respectively. In patients with mild hepatic steatosis, such as ours, decreased liver attenuation can appear similar to the spleen. To reduce incorrect diagnoses non-invasively, color doppler can confirm the presence of hepatic and portal veins in the left upper quadrant of the abdomen to differentiate between liver and spleen.