Abstract
Introduction: Spontaneous pneumomediastinum (SPM) is a rare clinical condition characterized by the presence of air or gas within the mediastinal tissue, without a history of recent trauma or iatrogenic cause. The condition presents with chest pain, dyspnea, and subcutaneous emphysema. Although SPM is generally a benign and self-limiting condition, it can lead to life-threatening complications in rare cases. We present a 25-year-old male patient with sudden onset of chest pain and dyspnea, who was diagnosed with SPM based on clinical examination, chest X-ray, and computed tomography (CT) scan. This highlights the importance of considering SPM as a differential diagnosis in patients presenting with chest pain and dyspnea, and the need for prompt and accurate diagnosis and management.
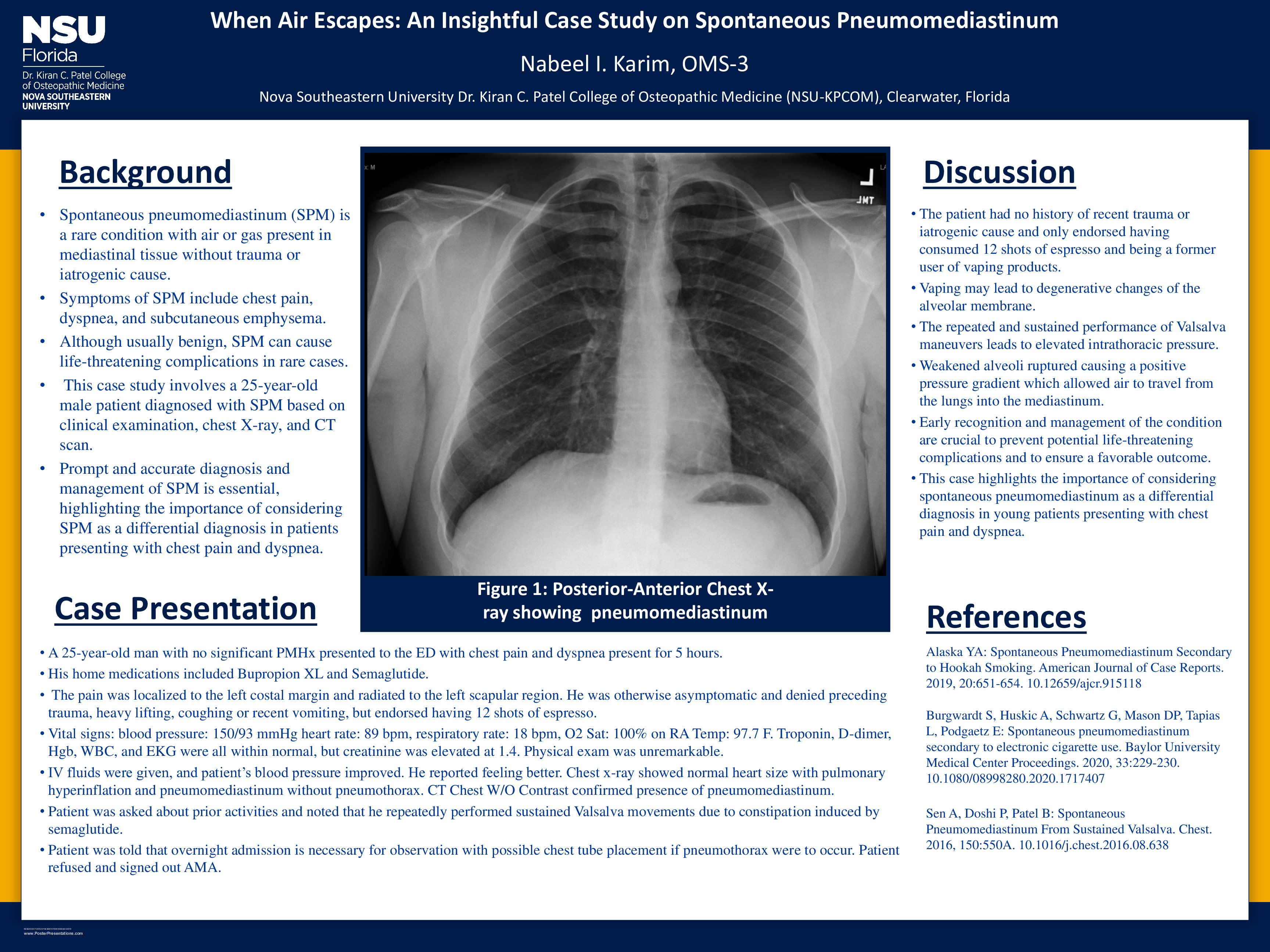
Case: A 25-year-old man presented to the emergency department with chest pain and dyspnea present for 5 hours. It was localized to the left costal margin and radiated to the left scapular region. He was otherwise asymptomatic and denied preceding trauma, heavy lifting, coughing or recent vomiting, but endorsed having 12 shots of espresso. He had no significant medical history, was a prior vape user on Bupropion Xl and Ozempic. His vital signs were: blood pressure 150/93 mmHg, heart rate 89 bpm, respiratory rate 18 bpm, oxygen saturations on room air 100% and temperature 97.7 F. Examination was also unremarkable. Troponin, d-dimer, Hgb, WBC, and EKG were all within normal, but creatinine was elevated. IV fluids were given and the patient’s blood pressure improved and reported feeling better. Chest x-ray showed normal heart size with pulmonary hyperinflation and pneumomediastinum without pneumothorax. CT Chest W/O Contrast confirmed presence of pneumomediastinum. Patient was asked about prior activities and noted being extremely constipated and repeatedly performed sustained Valsalva movements. The patient was told that overnight admission is necessary for observation with possible chest tube placement if pneumothorax were to occur. Patient refused, signed out AMA, and was advised to follow up with repeat Chest X-ray after one week or to return if condition worsens.
Discussion: Pneumomediastinum is a condition characterized by the presence of air or gas within the mediastinal tissue and can result from various causes such as trauma, iatrogenic procedures, spontaneous rupture of the alveoli or esophagus, and recreational drug use. However, in this case, the patient had no history of recent trauma or iatrogenic cause and only endorsed having consumed 12 shots of espresso and being a former user of vaping products. Repeated performance of Valsalva maneuvers leads to elevated intrathoracic pressure which lead to rupture of alveolar membrane causing positive pressure gradient of air from lungs into the mediastinum. This suggests that the patient's pneumomediastinum may have been caused by spontaneous alveolar rupture, a condition known as spontaneous pneumomediastinum.
The patient was treated conservatively with IV fluids. His blood pressure improved and reported feeling better. Despite this improvement, the patient was advised to undergo overnight observation but refused and signed out against medical advice.
It is important to consider spontaneous pneumomediastinum as a differential diagnosis in patients presenting with chest pain and dyspnea. Early recognition and management of the condition are crucial to prevent potential life-threatening complications.