Abstract
INTRODUCTION:
McCune-Albright syndrome is a rare heterogeneous, clinical condition caused by a rare genetic mutation in the GNAS1 gene recognized by the triad of polyostotic fibrous dysplasia, precocious puberty, and cafe-au-late spots. Exact incidence of McCune-Albright syndrome (MAS) is unknown. Its prevalence is probably between 1 in 100,000 to 1 case in 10,000,000 population. Therefore it is a very rare sporadically occurring disorder. Prognosis varies based on clinical manifestations of MAS.
CASE PRESENTATION:
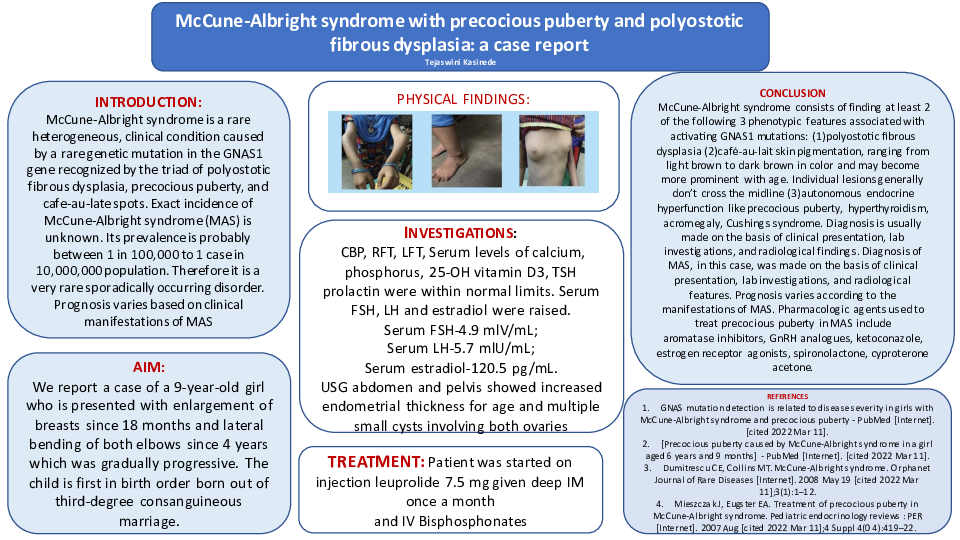
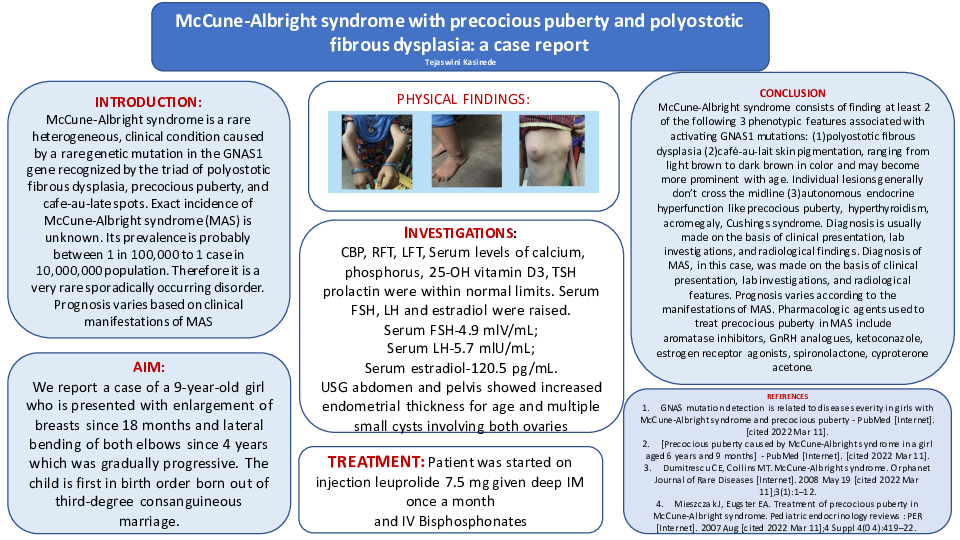
We report a case of a 9-year-old girl who is presented with enlargement of breasts since 18 months and lateral bending of both elbows since 4 years which was gradually progressive. The child is first in birth order born out of third-degree consanguineous marriage. The investigations done are,CBP, RFT, LFT, Serum levels of calcium, phosphorus, 25-OH vitamin D3, TSH prolactin were within normal limits. Serum FSH, LH and estradiol were raised. Serum FSH-4.9 mlV/mL; Serum LH-5.7 mlU/mL; Serum estradiol-120.5 pg/mL. USG abdomen and pelvis showed increased endometrial thickness for age and multiple small cysts involving both ovaries. Patient was started on injection Leuprolide 7.5 mg given deep IM once a month and intravenous Bisphosphonates
CONCLUSION
McCune-Albright syndrome consists of finding at least 2 of the following 3 phenotypic features associated with activating GNAS1 mutations: (1)polyostotic fibrous dysplasia (2)café-au-lait skin pigmentation, ranging from light brown to dark brown in color and may become more prominent with age. Individual lesions generally don’t cross the midline (3)autonomous endocrine hyperfunction like precocious puberty, hyperthyroidism, acromegaly, Cushings syndrome. Diagnosis is usually made on the basis of clinical presentation, lab investigations, and radiological findings. Diagnosis of MAS, in this case, was made on the basis of clinical presentation, lab investigations, and radiological features. Prognosis varies according to the manifestations of MAS. Pharmacologic agents used to treat precocious puberty in MAS include aromatase inhibitors, GnRH analogues, ketoconazole, estrogen receptor agonists, spironolactone, cyproterone acetone.