Abstract
IgA nephropathy is the principal cause of ESRD and most common form of glomerulonephritis. It may present in a variety of ways with multiple therapeutic options. This is a peculiar case of a young patient with no pertinent past medical history who presents with rapid onset of IgA nephropathy causing ESRD.
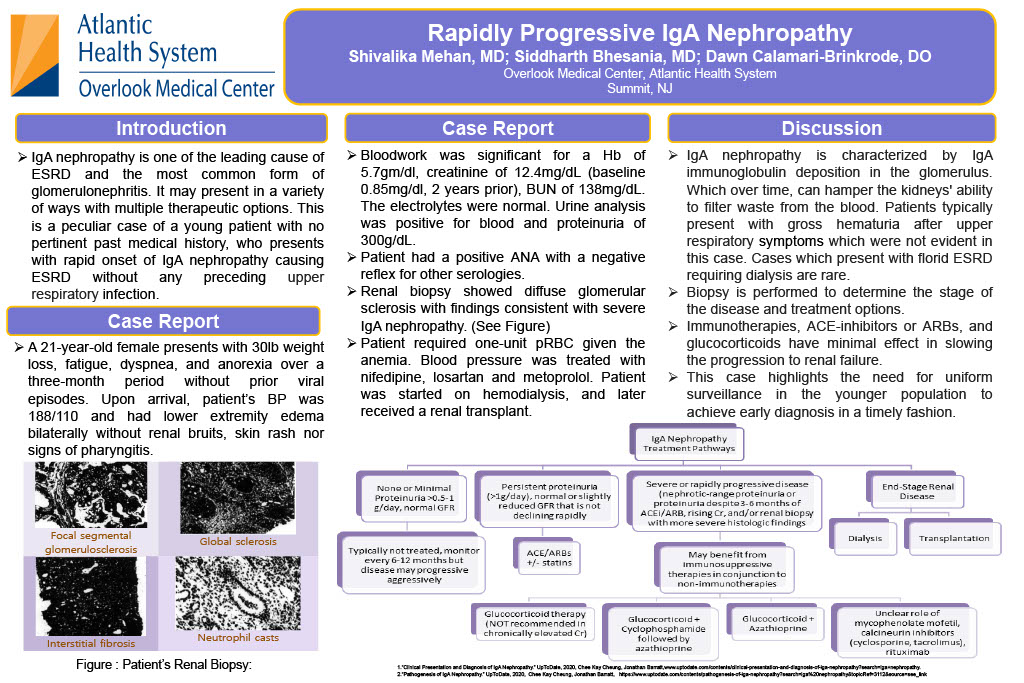
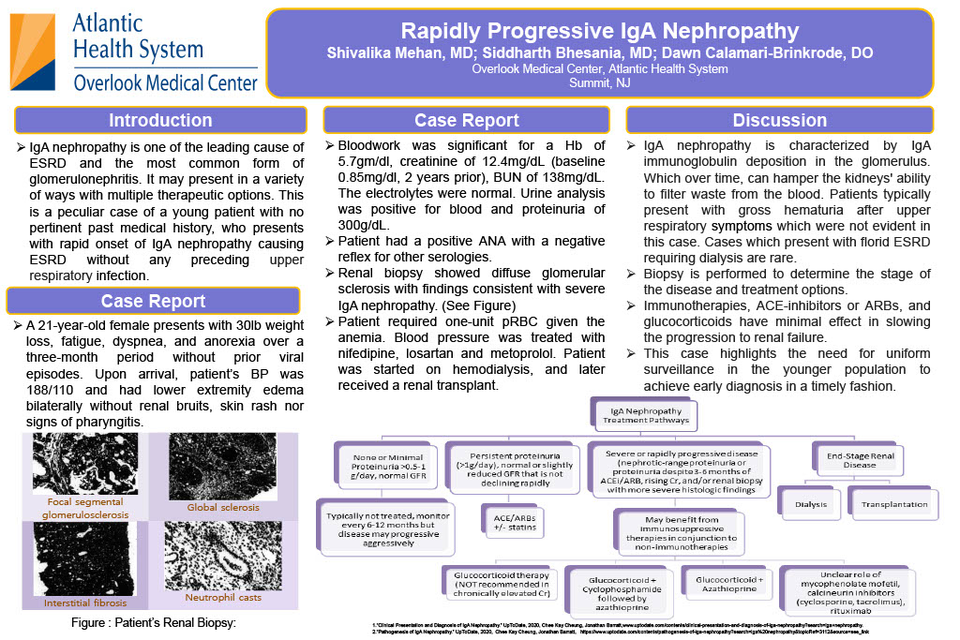
A 21-year-old female presents with 30lb weight loss, fatigue, dyspnea, and anorexia over three-month period with no preceding viral episodes. Upon arrival, patient’s BP was 188/110 and had lower extremity edema bilaterally but no renal bruit, skin rash, and signs of pharyngitis. Bloodwork was significant for Hb 5.7 for which she required blood transfusions, creatinine of 12.4, BUN of 138, normal electrolytes. UA was positive for blood and proteinuria of 300.Patient's past medical records showed a creatinine of 0.85. Patient had a positive ANA with a negative reflex for other serologies. Renal biopsy showed diffuse glomerular sclerosis with findings consistent with severe IgA nephropathy (Figure 1-4). She was treated with nifedipine, losartan and metoprolol; started on hemodialysis and eventually, received renal transplant.
IgA nephropathy is characterized by IgA immunoglobulin deposition in the glomerulus, the IgA nephropathy cases which present with florid ESRD requiring dialysis are rare. Patients usually present with gross hematuria after an upper respiratory tract. Biopsy is performed to determine the stage of the disease and treatment options. Immunotherapies, ACE-inhibitors/ARBs, glucocorticoids have shown to prove very minimal effect in slowing the progression. The significance of this case is to highlight need for a uniform surveillance in particular patient populations to achieve early diagnosis in a timely fashion to avoid cases as these as disease progression was chronic in nature demonstrated by her shrunken kidney size and the disease already progressed to the end stage requiring dialysis.