Abstract
Introduction
Dieulafoy’s lesion is a rare vascular malformation of the gastrointestinal tract, first described by Paul George Dieulafoy in 1898, it is also called aneurysm of the gastric vessels.It is normally present in the stomach and more rarely in the colon and is responsible for 2% to 6.5% causes of all gastrointestinal bleeding.It presents with sudden onset severe gastrointestinal hemorrhage and can occur in people of all age groups. Symptoms may include hematemesis, melena stools, hematochezia, hemoptysis with or without signs of hemodynamic derangement.
Case Description
A 30 year old African male who presented to the ER with an episode of moderate to severe bright red blood loss per rectum of six hours duration. He worked as a long distance truck driver with no history of smoking,Alcohol use,NSAIDS use or previous surgical history.He has a past medical history of Symptomatic third degree external hemorrhoid which was managed conservatively.His rectal bleeding was acute in onset,sudden and not preceded by abdominal pain, vomiting or trauma to any part of the body.
Vital signs on presentation were T:97.7 F, BP:90/70 mm Hg, RR:18cpm and HR:96bpm.Physical examination revealed an ill appearing mildly pale young male patient with tachycardia and tachypnea. Abdominal examination was unremarkable.Digital rectal examination revealed a third degree external hemorrhoids and a second degree internal hemorrhoids just above the pectinate line with fresh blood clots.
Notable laboratory findings were Hb:9g/dl,WBC:8.3x103,Hematocrit:28%,MCV:70fl,MCHC:24g/dl,Ferritin:10mcg/dl,serum iron level:50 mcg/dl,TIBC:600mcg/dl and transferrin saturation percentage:60%.The patient was supportively managed with intravenous crystalloid fluid.A consult was written to the gastroenterology and surgical team and one unit of fresh whole blood was transfused.
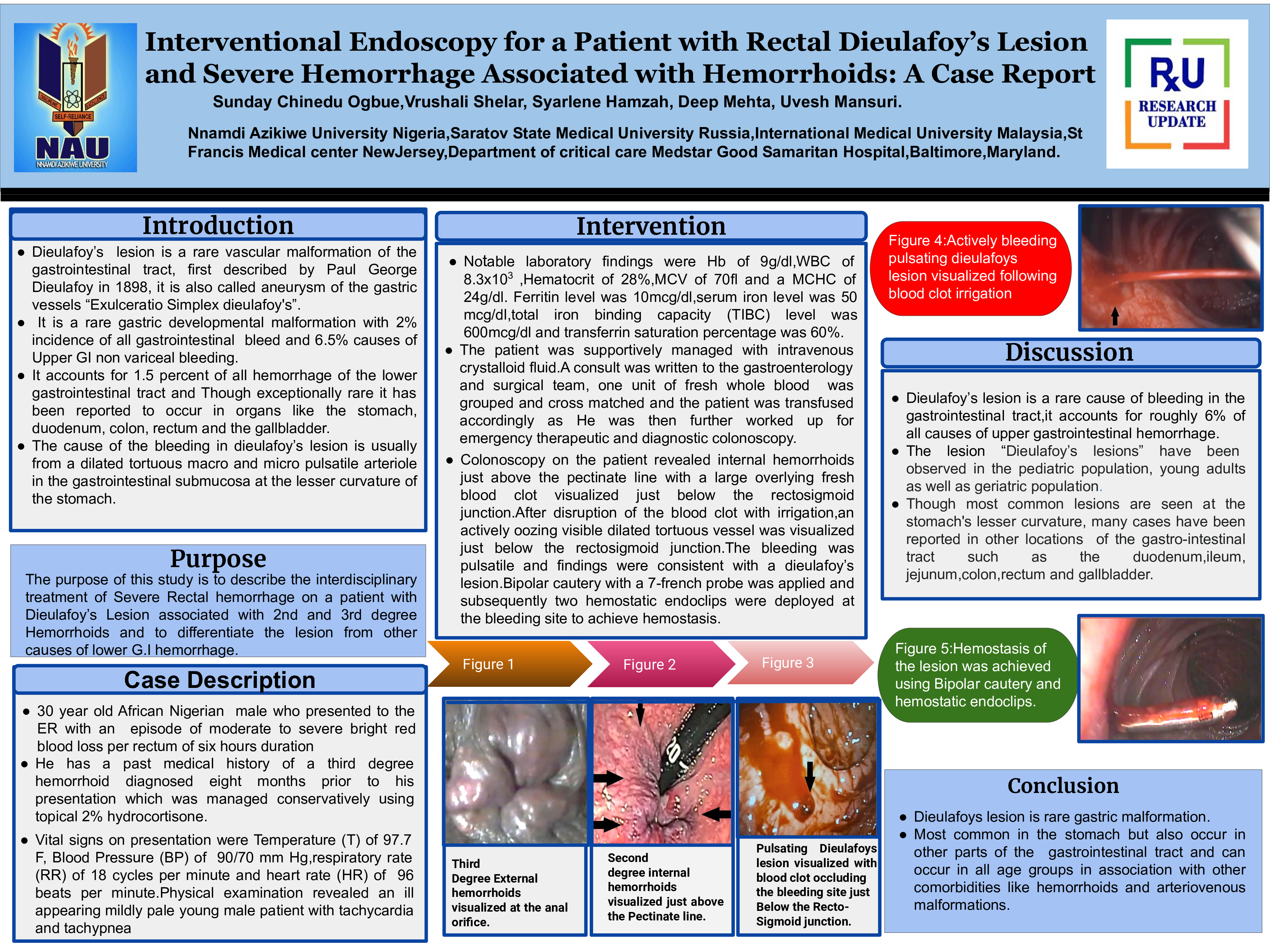
Colonoscopy revealed internal hemorrhoids just above the pectinate line with overlying fresh blood clot visualized just below the rectosigmoid junction. Irrigation of the blood clot revealed an actively bleeding pulsating tortuous vessel just below the rectosigmoid junction with findings consistent with a dieulafoy’s lesion.Bipolar cautery with a 7-french probe was applied and two hemostatic endoclips were deployed at the site to achieve hemostasis
Discussion
The diagnosis of dieulafoy's lesion is uncommon and difficult because it is a rare condition.Due to its varied nature among different age groups and varied location the lesion should be considered as part of a differential diagnosis for gastrointestinal bleeding,The cause of the lesion is not yet known however different theories have been proposed. Iron deficiency anemia and chronic anemia are rarely associated with dieulafoy's lesion except in cases where there is associated comorbidities like hemorrhoids, arteriovenous malformations and neoplasms.In the event of severe gastrointestinal bleeding the treatment options for dieulafoy’s lesion includes emergency endoscopy and colonoscopy and for patients who fail to achieve primary hemostasis other treatment options like surgery should be considered.
Conclusion
Dieulafoy’s lesion is rare a gastric malformation and can occur in all age groups.It is important to differentiate the lesion from associated comorbidities when present through interventional and diagnostic endoscopy as doing so have proven to be effective with an increase treatment success rate.