Abstract
Objectives: To evaluate the accuracy of intracranial frameless stereotactic radiosurgery (SRS) and stereotactic radiotherapy (SRT) using the Encompass mask immobilization system, cone beam computed tomography (CBCT), six degrees of freedom (6DoF) couch, and optical surface monitoring system (OSMS).
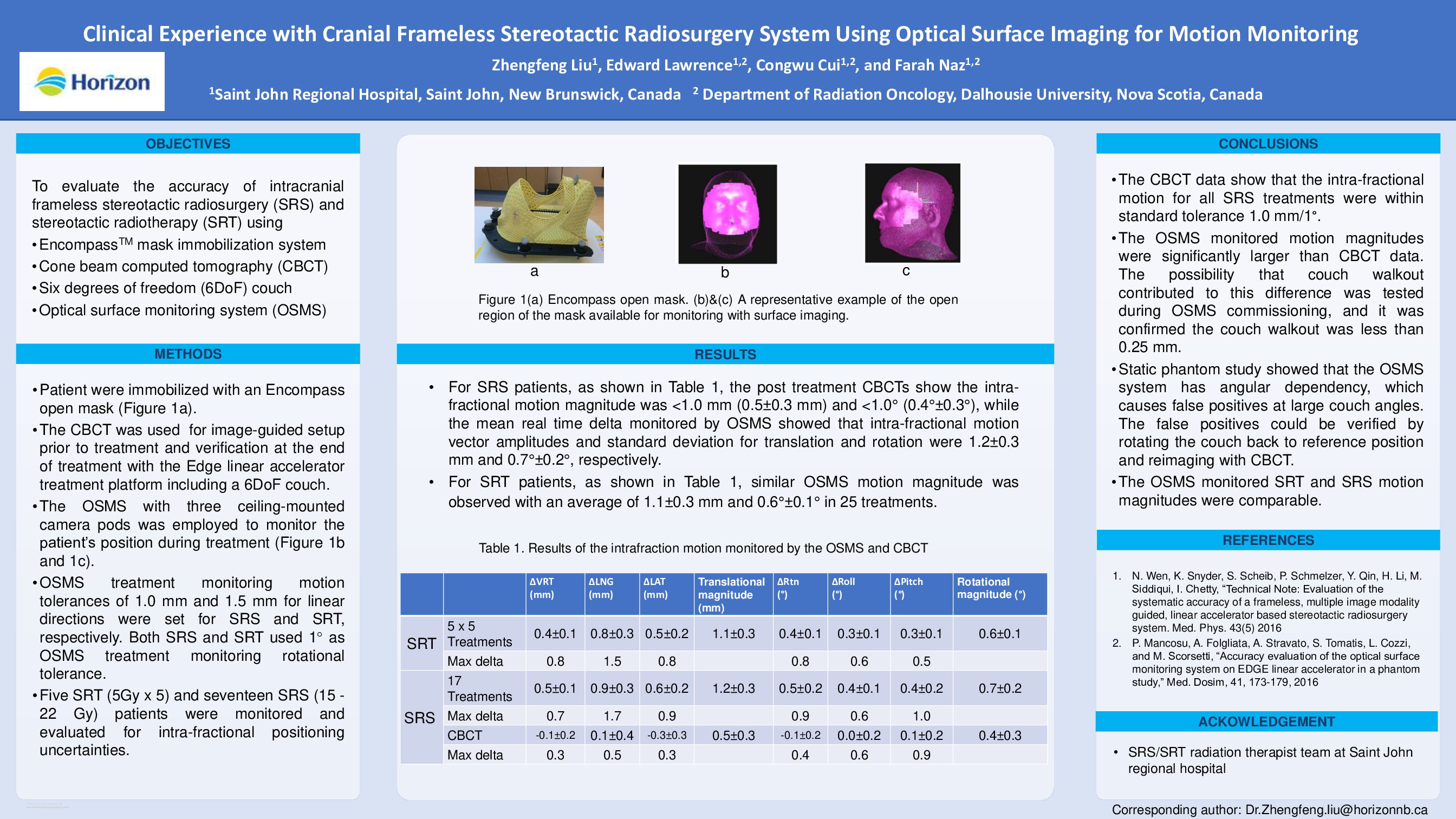
Methods: Patients were immobilized with an Encompass open mask which allows the OSMS to monitor the patient's skin surface in real-time. The OSMS with three ceiling-mounted camera pods was employed to monitor the patient's position prior to, and during treatment at multiple treatment couch angles. The CBCT was used as the standard for image-guided setup with the Edge linear accelerator treatment platform including a 6DoF couch. Motion tolerances of 1.0 mm and 1.5 mm for linear directions were set for SRS and SRT, respectively. Both SRS and SRT used 1° as rotational tolerance. These tolerances were set to ensure head motion remained within the treatment margin during beam on periods. At the end of treatment, the couch was returned to the reference position and a final CBCT was taken for comparison with the setup CBCT. Five hypo fractionated (5Gy ×5) frameless SRT, and seventeen single fraction (15-22 Gy) frameless SRS patients were monitored and evaluated for intra-fractional positioning uncertainties.
Results: For SRS patients, the post treatment CBCTs show the intra-fractional motion magnitude was <1.0 mm (0.5±0.2 mm) and <1.0° (0.3°±0.1°), while the mean real time delta monitored by OSMS showed that intra-fractional motion vector amplitudes and standard deviation for translation and rotation were 1.2±0.3 mm and 0.7°±0.2°, respectively. For SRT patients, similar OSMS motion magnitude was observed with an average of 1.1±0.3 mm and 0.6°±0.1° in 25 treatments.
Conclusions: The CBCT data show that the intra-fractional motion for all SRS treatments were within standard tolerance 1.0 mm/1 degree. The OSMS monitored motion magnitudes were significantly larger than CBCT data. The investigation of OSMS commissioning confirmed the couch walkout was within 0.25 mm. Static phantom study showed that the OSMS system has angular dependency, which causes false positives at large couch angles. The false positives could be verified by rotating the couch back to reference position and reimaging with CBCT. The OSMS monitored SRT and SRS motion magnitudes were comparable. The planning target volume (PTV) margin for SRT treatments needs further analysis and investigation.