Abstract
Introduction: Calciphylaxis is a rare disease that involves calcifications of the arterioles, especially for those who have end-stage kidney disease (ESKD). Hyperphosphatemia and warfarin are major risk factors. It involves arteriolar medial layer calcification and subintimal fibrosis leading to thrombosis and ischemia. Calciphylaxis, also known as calcific uremic arteriolopathy, presents with a poor prognosis in patients on dialysis as it increases the mortality rate by three times. There are several reports on calciphylaxis; however, no reports explain the exact pathophysiology. This disease is important as many healthcare providers are not aware of its manifestations, especially when it can occur in patients with ESKD and warfarin, a common disease and a commonly prescribed medication. It is crucial for physicians to do a thorough physical examination as well as closely monitor labs as these can hint towards calciphylaxis
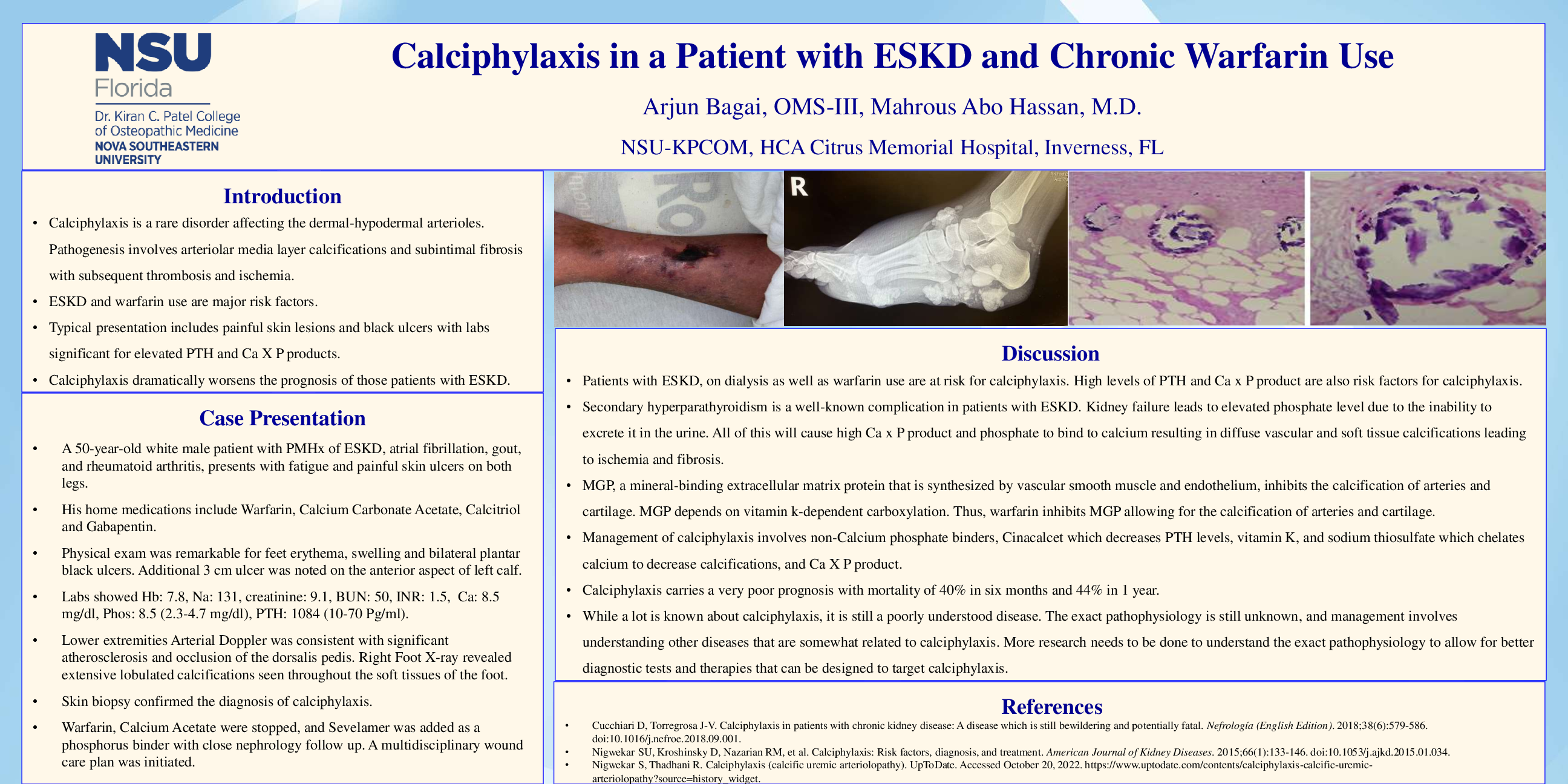
Case Description: A 50-year-old white male patient presented to the ED with black, painful ulcers on both lower extremities. He complained of fatigue, weakness, and nausea. His past medical history is significant for atrial fibrillation, ESKD, gout, and rheumatoid arthritis. His past surgical history is significant for AV fistula of the left upper extremity and peritoneal catheter placement. His home medications include warfarin, calcium carbonate acetate, calcitriol, and gabapentin. Physical examination was remarkable for feet and leg erythema, swelling, and bilateral black plantar ulcers. An additional 3 cm ulcer was noted on the anterior aspect of the left calf. Labs were significant for anemia, elevated creatinine and blood urea nitrogen, hyperphosphatemia, and hyperparathyroidism. Lower extremity arterial doppler showed calcific occlusion of the dorsalis pedis vessels and histopathology of the skin is consistent with the diagnosis. Warfarin was stopped, a non-Calcium-Phosphate binder was started, and wound care was initiated. After a couple of weeks, he was discharged to a nursing home facility in a stable condition.
Discussion: The diagnosis of calciphylaxis is primarily clinical, with histopathology and imaging assisting with the diagnosis. Management involves a multidisciplinary approach involving primary care, nephrology, dermatology, palliative care, and pain specialists. While there is no cure or definitive treatment, some agents, such as sodium thiosulfate, Vitamin K, and SNF472 show some effectiveness in calciphylaxis management. Calciphylaxis, while described merely as a calcification dilemma, is more complicated based on the presence of different mediators and different pathogenic features in arterioles. Further research needs to be done to understand the exact pathophysiology of this disease; this will allow for a better understanding of treatments needed for successful management.