Abstract
Introduction and Objective:
Abdominal striae (striae distensiae) have many etiologies, including Cushing’s syndrome, exogenous steroid utilization, obesity, pregnancy, and puberty. Exogenous steroid use has been linked to abdominal striae, due to exogenous steroids causing a state of hypercortisolism. Abdominal striae caused by exogenous steroid use that causes the cortisol levels to remain at sub-physiological levels (hypocortisolemia) has never been reported. The objective of this case report is to highlight the importance of informing patients about the side-effects associated with steroid utilization, even at low doses, to prevent them from experiencing psychological alarm.
Case presentation:
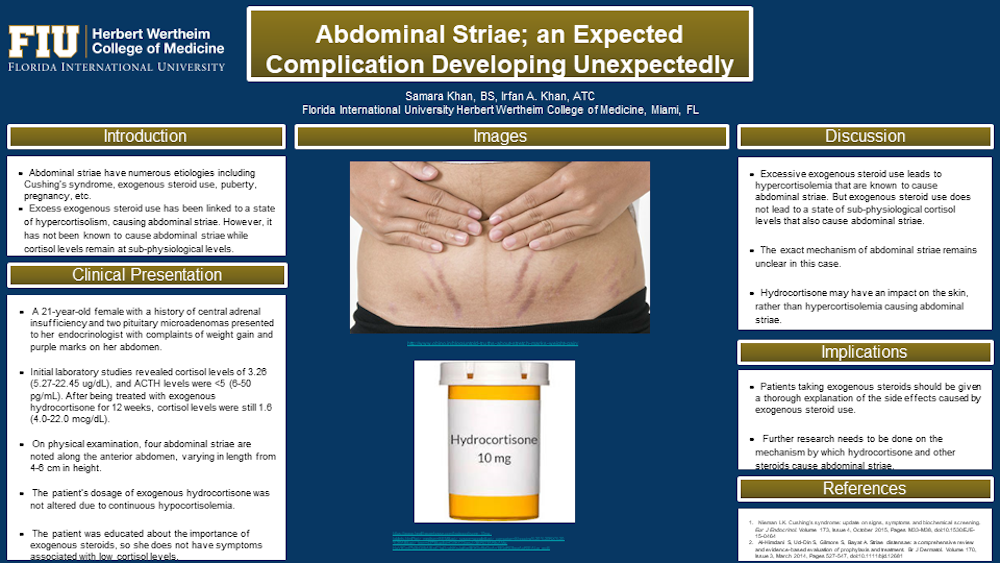
A 21-year-old female, with a history of central adrenal insufficiency and two pituitary microadenomas (2mm and 1mm), presented to her endocrinologist’s office with complaints of weight gain and purple marks on her abdomen. The symptoms began within two weeks of starting hydrocortisone therapy (20 mg at 7am, 10 mg at 7pm), and the marks increased in quantity and size for the following 10 weeks. Upon physical examination of the abdomen, four abdominal striae were observed along the anterior abdomen, varying from 4-6 cm in height. The striae were not tender to palpation. Upon being diagnosed with central adrenal insufficiency, the patient’s initial cortisol levels were 3.26 (5.27-22.45 ug/dL), and ACTH levels were <5 (6-50 pg/mL). After being treated for 12 weeks, the patient’s fasting morning cortisol level was only at 1.6 (4.0-22.0 mcg/dL). A diagnosis of abdominal striae secondary to hydrocortisone therapy was made. Since the patient still had hypocortisolemia, even with compliance to the hydrocortisone medication, the patient’s dosage of hydrocortisone was not altered. The patient was educated about the necessity of exogenous steroids, so she does not have symptoms associated with low cortisol levels such as postural hypotension. While frustrated with the abdominal striae, she was motivated to exercise and eat a better diet to lose weight.
Conclusions-Implications:
While current literature says that elevated levels of cortisol, caused by chronic exposure to exogenous steroids, can cause abdominal striae, we are reporting an unusual and rare case where a hypo-physiological dose of hydrocortisone caused abdominal striae rapidly. This supports that hydrocortisone and other steroids may have a direct impact on the skin, rather than the hypercortisolemia causing abdominal striae. It is imperative for clinicians to educate their patients about the side effects of medications they are taking, and to perform physical examinations on patients to screen for the presence of these side effects. Further research needs to be performed to discover the exact mechanism by which hydrocortisone and other steroids cause abdominal striae.